Rotator cuff injuries are one of the most common causes of shoulder pain. Fortunately, rotator cuff problems can be successfully treated with osteopathy, and exercises (avoiding overhead activities) advised by an osteopath or physiotherapist. Occasionally, steroid injections or surgery is required.
What is the rotator cuff?
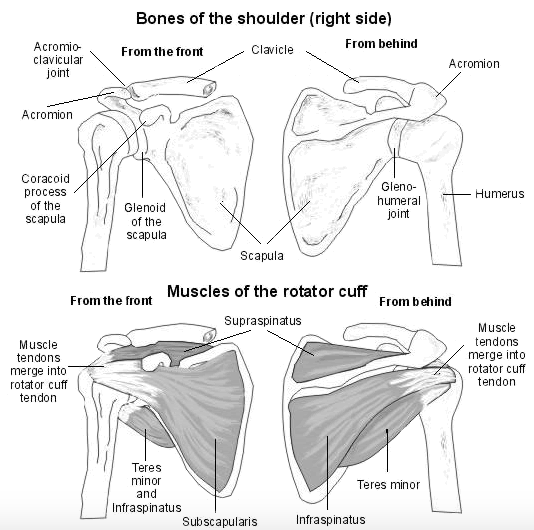
The rotator cuff is a group of four muscles that stabilises the gleno-humeral joint, i.e. the ball-in-socket joint of the shoulder.
The muscles are:
- supraspinatus
- infraspinatus
- teres minor
- subscapularis
In addition to stabilising the gleno-humeral joint, the rotator cuff muscles are responsible for movement of the humerus relative to the shoulder blade.
So if you have a rotator cuff injury, your shoulder may become unstable, and you may find it difficult to do certain movements.
The tendons of the rotator cuff muscles pass under the subacromial space and attach to the humeral head. The subacromial space is a narrow space containing a pain-sensitive fluid-filled sac, called a bursa.
The purpose of a bursa is to reduce friction. If there is any inflammation or thickening of the tendons under the subacromial space, the bursa becomes irritated and there is pain.
Subacromial pain is especially felt between 60 and 120° of shoulder abduction. This is because, anatomically, the subacromial space is at its smallest in this range. Between 60 and 120°, the bursa is at increased risk of being irritated. This holds especially true if injury to the rotator cuff muscles has lead to inflammation or tendon thickening. If there is pain in this range, there is subacromial impingement. Clinically, this range is called the painful arc.
Together with the range of movement tests, palpation, and muscle tests, painful arc is used to diagnose rotator cuff injury.
If more information is needed, e.g. to determine whether there is a full rupture of a tendon, ultrasound sonography is the gold standard. Ultrasound scans are cheap and highly diagnostic and, for these types of shoulder problems, better than MRI.
What causes rotator cuff injury?
Rotator cuff injury is a broad term – it covers muscle tears and ruptures, tendinopathies, and calcific tendinitis.
All have in common a form of degeneration that is often due to repetitive strain, inflammation, or age-related changes. And all lead to subacromial impingement.
In fact, anything that compromises the rotator cuff or occupies the subacromial space – be it swelling due to osteoarthritis, or bone spurs – can lead to subacromial impingement.
Rotator cuff tears
The rotator cuff muscles that are most vulnerable to tears are the suspraspinatus and subscapularis. Tears can develop gradually or be caused by a single impact to the shoulder.
Tendon tears can be minor/partial or full/complete. Small tears tend to be more painful than large tears. To ascertain the extent of tendon injury, both ultrasound and MRI scans can be used. Yet, not only are ultrasound scans cheaper, but – for this purpose – better.
A full rupture of the tendon can be surgically reconstructed. However, this is only recommended in young patients who participate in sports that require full functioning of the rotator cuff.
Supraspinatus tendinopathy
Supraspinatus tendinopathy, or tendinitis, is a thickening of the supraspinatus tendon in response to repetitive strain or overuse. The aforementioned confined space in the subacromial space, especially when the shoulder is between 60 and 120°, leads to irritation of the subacromial bursa (i.e. bursitis) if there is tendon thickening or general swelling.
Calcific tendonitis
In calcific tendonitis, calcium accumulates in the tendons of rotator cuff muscles. The deposited calcium takes up extra space under the acromion, and can even replace tendon.
Calcification is more common in patients between 40 and 60 years of age and increases the risk of subacromial impingement. Shoulder calcification can resolve without treatment.
What are the symptoms of rotator cuff disorders?
Rotator cuff disorders are characterized by pain in and around the gleno-humeral joint of the shoulder. There is often pinpoint pain over the deltoid tubercle and in the anterolateral arm. Sometimes the pain radiates along the biceps as referred pain.
Pain will be worse on movement, especially in the painful arc, i.e. during 60 to 120° abduction. There may be weakness, instability, and, therefore, clicking. Your pain may be worse at night.
You may find it difficult to comb your hair, iron, put on a coat, swim, paint, and, if you’re a woman, putting your bra on. Writing and typing should feel fine, because these movements are more dependent on the forearm muscles.
How can I help rotator cuff disorders?
First of all, avoid activities that aggravate the pain. Taking pain-killers can make this difficult, because you are masking the pain.
Rest
If possible, avoid overhead activities, such as tennis, playing cricket, painting, plastering, and decorating. This is because overhead activities reduce the subacromial space and make impingement likely.
While the shoulder is acute, you should allow it time to rest and recover. Listen to your body. However, you must not completely immobilise your shoulder for too long.
Exercises
I often show patients an exercise that osteopaths call ‘pendulum’: It involves mobilising your shoulder by letting it dangle in a pendular fashion. It is a great exercise because it relies on gravity and achieves safe movement with minimal effort.
Once the shoulder is less acute, you can start gently strengthening your shoulder. These should be very gentle exercises. I recommend using a thera-band and concentrically and eccentrically contracting your rotator cuff muscles. An osteopath or physiotherapist can show you how. Any exercise that causes discomfort should be avoid. Pain indicates you are moving too fast.
Acupuncture
An acupuncturist can treat local shoulder points, and LI4, LI15, SI3 and SI10.
Massage
A massage therapist can treat associated trigger points and muscles.
Painkillers
Painkillers, such as paracetamol, and anti-inflammatory painkillers, such as ibuprofen, naproxen and diclofenac, can reduce the pain. However, I am not a huge fan because painkillers often obfuscate the clinical picture. You might think your shoulder is better than it is and further damage the tissues. I personally would only take painkillers if the pain is unbearable or preventing me from sleeping.
In addition to confusing the clinical picture, painkillers can also cause side effects.
If you want to reduce local inflammation and swelling, ice packs or frozen peas (wrapped in a towel) are useful.
Steroid injections
Steroid injections can be useful because they will reduce swelling, and therefore create more space under the acromion. However, because steroids are such strong drugs, it is recommended not to have more than two injections. And, if possible, more conservative approaches that go to the root of the impingement should be addressed first. Steroid injections only treat the symptom, not the cause.
Surgery
Surgery may be indicated if non-invasive approaches have been tried but the pain persists. Examples are reconstruction of rotator cuff tendons, arthroscopic decompression of the subacromial space, or removal of calcium.
Can osteopathy help rotator cuff disorders?
Rotator cuff injuries are rarely a quick fix. Recovery often takes significantly longer than six months, and some people press for surgery.
Fortunately, osteopathy can be very effective. I have seen many patients whose symptoms, with regular treatment, improved within 1–3 months.
I use advanced muscle testing techniques to determine which muscles are compromised, and work with all three shoulder joints to improve the mechanics of the shoulder. As an osteopath, I test for involvement of the spine, where the nerve supply to the shoulder muscles arises.
If you have mechanical shoulder pain, please get in touch.
To book an Osteopathy appointment in New Malden or in Marylebone, phone 020 8942 3148 or contact Aston Clinic London.
Aston Clinic London is a third-generation complementary health clinic based in New Malden and serves the local areas of Kingston, Wimbledon, Raynes Park, Surbiton, Chessington, Worcester Park, Sutton and other areas of southwest London and Surrey.
Aston Clinic London also offers Osteopathy and Herbal Medicine in Marylebone, Central London.